The Definitive Guide to Perimenopause & Mental Health
Edited & Reviewed by Kira Hensley, M.A., M.Ed., Registered Psychotherapist ~ Women's Mental Health, Anxiety & Perimenopause
Understanding the biological, emotional, and psychological shift
If you’re in your late 30s or 40s, and you’ve entered perimenopause and suddenly feel anxious, overwhelmed, irritable, exhausted, foggy, or simply “not like yourself,” you’re not alone! Perimenopause is a a reproductive transition that includes a biological and psychological shift that changes how your brain processes stress, emotion, sleep, and resilience. This guide will help you understand what’s happening, why it makes sense, and what support can actually help.
What this guide covers:
Inside, you’ll learn why perimenopause can affect:
your nervous system and stress response
anxiety (from worry to panic)
irritability and rage that feels “out of character”
low mood, depletion, and emotional flatness
sleep disruption, exhaustion, and brain fog
identity shifts, grief, and the sense that “something is changing”
what helps — including therapy, nervous-system support, and medical options
Table of contents (jump to a chapter)
I. The “Why”: What’s Happening to Me?
II. The Anxiety Spectrum: From Worry to Panic
III. Menopause Rage & Irritability
IV. Depression, Depletion, and Anhedonia
V. Sleep, Exhaustion, and Brain Fog
I. The “Why”: What’s Happening to Me?
If perimenopause has made you feel like a different person, it can be genuinely unsettling. Clients often describe it as waking up one day with a thinner emotional skin; they are more reactive, more sensitive, more easily overwhelmed, and they can’t explain why. You may find yourself thinking, “This isn’t me,” or “I used to handle everything,” or even “Am I falling apart?”
Perimenopause can create a very real sense of sudden internal change, and when it isn’t named, some women assume it means something is wrong with them.
Why do I feel so different?
Perimenopause is a neurobiological transition, not just a reproductive one. As hormones begin to fluctuate (especially estrogen and progesterone) the brain receives less predictable chemical input than it has for decades.
Progesterone gradually declines and often takes with it some of the nervous system’s natural “calming brake.” You might feel more tense, more easily overstimulated, or less able to settle.
Estrogen doesn’t simply drop; it often swings. Those fluctuations can affect neurotransmitters like serotonin and dopamine, which shape mood, motivation, and emotional steadiness.
Over time, there is a gradual decline in testosterone, which can influence energy, drive, confidence, and resilience.
At the same time, midlife often comes with a high cognitive and emotional load: work demands, caregiving, relationship strain, invisible mental labour, shifting roles. When the brain’s internal buffering changes but your external demands don’t, your threshold gets smaller. Reactions rise faster. Recovery takes longer. And the gap between stimulus and response can feel thinner than it used to.
Your nervous system is adapting in a new internal environment.
Hormones & the Brain: How Shifting Chemistry Shapes Your Mental Health
Menopause is often described as a hormonal transition, but what most women aren’t told is that it is also a neurological one. The hormones that fluctuate during perimenopause affect the brain circuits responsible for mood, focus, memory, sleep, stress tolerance, energy, and emotional steadiness. When these hormones change, the brain changes with them.
Understanding this connection can be incredibly grounding. Women often feel immediate relief when they realize, “Oh… it’s not just me. There’s a real reason for this.”
Hang on with me as we dive into a little biology.
Progesterone: The Calming Cushion That Begins to Disappear
Progesterone supports the brain’s main calming system: the GABA pathway. When progesterone is steady, women often feel more settled inside, more buffered against stress, and more able to sleep and regulate emotions.
During perimenopause, progesterone is usually the first hormone to decline, and it declines early and steadily. Without it, women notice they feel more on edge, more easily overwhelmed, more irritable, and less able to access that sense of inner calm they once took for granted. Your brain has lost the calming influence it relied on for decades, and you’re having to figure out how to cope without it.
Estrogen: Not “Good” or “Bad,” But Highly Influential
If progesterone is the calming hormone, estrogen is the complex communicator. It influences serotonin (mood), dopamine (motivation and focus), acetylcholine (memory and learning), and even the brain’s blood flow and energy use.
But estrogen doesn’t simply decline in perimenopause — it swings, and sometimes dramatically. These swings can create emotional and cognitive instability that feels unpredictable: a good day followed by a shaky one, or moments where your mood or clarity shift without warning.
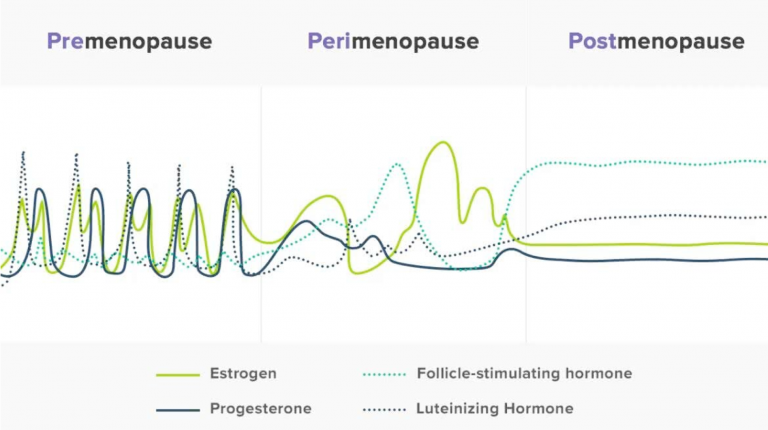
The hormonal chaos of Perimenopause (picture retrieved from Flordis.com.au)
Testosterone: Motivation and Confidence
Though less talked about, testosterone plays a role in women’s motivation, assertiveness, focus, libido, and even that inner sense of “drive.” Levels naturally decrease with age, and some women begin to feel that drop during perimenopause. It’s often a sense of having less spark, less initiative, or less mental momentum than before.
It can feel like losing your “get up and go,” even in areas you used to feel naturally energized.
Cortisol and Neurotransmitters
The hormonal shifts of midlife also change how the stress system behaves. Cortisol spikes more easily, emotional recovery takes longer, and the nervous system becomes more reactive. This is why women who have been resilient their entire lives suddenly feel more sensitive to stress or overwhelmed by situations they once handled easily.
Because hormones regulate neurotransmitters, changes in estrogen and progesterone ripple out into the systems that control mood, anxiety, sleep, focus, and memory. When these chemical messengers become less predictable, it’s normal to feel:
more anxious or unsettled
more prone to low or flat mood
less motivated
more sensitive or reactive
less able to concentrate or remember things
Your brain is adjusting to an entirely new hormonal environment.
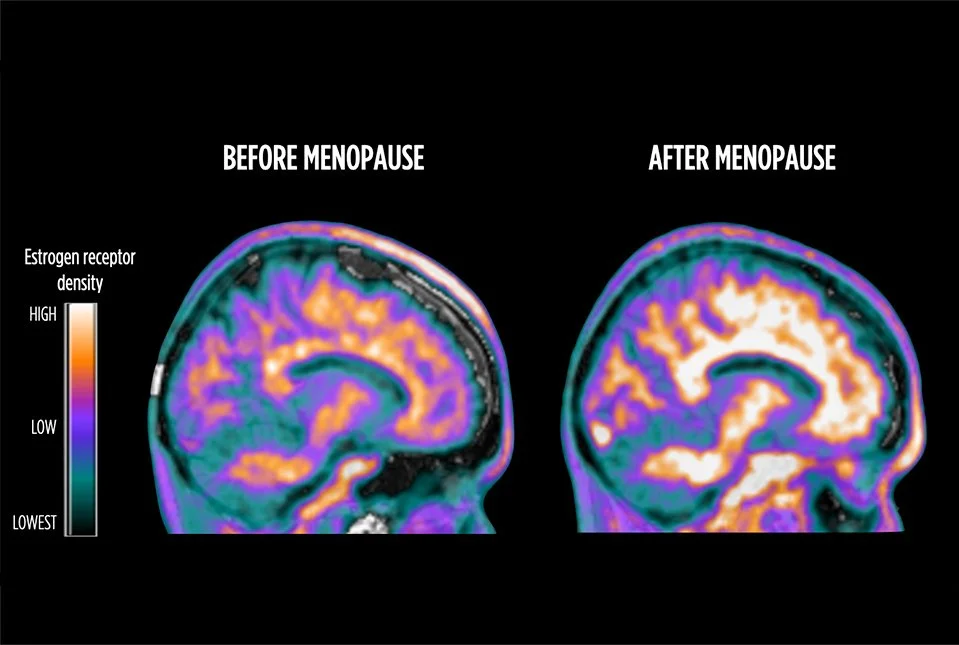
Mosconi Lab. Scans Show Brain's Estrogen Activity Changes During Menopause. (2024). Retrieved from Weill Cornell Medicine Newsroom.
The brain attempts to make up for the declining estrogen by increasing the number of estrogen receptors in the brain’s cells.
The Combined Effect: A Nervous System With Less Cushion
When you put all of this together, the nervous system becomes more sensitive, less buffered, and more easily overwhelmed. Things that once felt simple now feel harder. Stressors that once barely registered now hit sharply. Cognitive effort increases. Emotional steadiness decreases.
These changing internal supports often destabilizes the coping strategies women have relied on for decades. Women who are highly capable, productive, conscientious, and used to managing everything suddenly find that the same level of effort no longer produces the same outcome. The nervous system has less reserve and recovery takes longer. The “push through it” strategy stops working.
And Here’s the Good News: The Brain Stabilizes Again
Once you reach post-menopause, hormone levels settle into a more consistent pattern. Often, emotional intensity softens and cognitive clarity returns. The transition is the turbulent part. And your brain is doing its best to adapt!
Meanwhile, How do I Cope?
The first step is reframing: treat these shifts as information. In therapy, we can:
map your most common triggers (overstimulation, conflict, sleep loss, over-responsibility)
identify where your capacity has changed, and where your life still expects your “old capacity”
build nervous-system supports (pacing, boundaries, rest, and targeted coping tools)
reduce shame and self-criticism
coordinate with medical care when symptoms suggest hormonal or sleep interventions could help
You don’t need to “push through” to prove you’re strong. You need a framework that makes sense, and support that helps you adapt without losing yourself.
For a Closer Look:
What’s Happening to My Brain? Why Perimenopause Makes You Feel Like You’re Losing It (biological “why” guide)
Perimenopause & Emotional Sensitivity: Why Everything Feels Personal Now (why your emotional skin feels thinner)
What the Research Shows
What we know:
The menopause transition can be a window of vulnerability for mood symptoms in some women, including new-onset or recurrent depression (source: Menopause Society Menopause Topics: Mental Health & Menopause Society Menopause Topics: Perimenopause)
Sleep disruption and vasomotor symptoms (like night sweats) can fragment sleep, and poor sleep reliably worsens anxiety, irritability, mood, and concentration (source: Society of Obstetricians & Gynaecologists of Canada Menopause: Mood, Sleep & Cognition)
Mental health symptoms in perimenopause are common and can include anxiety, low mood, irritability, brain fog, and lowered self-esteem — even for women with no prior mental health history (source: Beyond Blue Australia)
Effective support is often multi-layered: addressing sleep, stress physiology, psychological coping patterns, and (when appropriate) medical options (source: Society of Obstetricians & Gynaecologists of Canada Clinical Practice Guideline)
What we’re still learning (and why it matters):
Exactly who will be most affected by hormone fluctuations (some women are more sensitive than others), and which specific mechanisms drive symptoms for each individual (source: Menopause Society)
The best “matching” of treatments to symptom profiles, for example, who benefits most from hormone therapy, psychotherapy, antidepressants, or combined approaches Society of Obstetricians & Gynaecologists of Canada Clinical Practice Guideline and Menopause Journal: Consensus Recommendations: Guidelines for the evaluation and treatment of perimenopausal depression).
II. The Anxiety Spectrum: From Worry to Panic

Women who never had difficulty driving are often surprised when it becomes anxiety-provoking in perimenopause.
If anxiety has shown up in perimenopause, especially if you’ve never been an “anxious person,” it can feel confusing and scary. A common experience is a sense of being “on alert,” a tight chest or buzzing body, or sudden spikes of panic that seem to come out of nowhere. Clients have described to me sitting in parking lots before work trying to manage their panic. Others notice their worries getting louder and stickier, as if their mind can’t stop scanning for what might go wrong.
When your anxiety feels disproportionate to your life circumstances, it’s easy to assume you’re losing resilience. More often, what’s happening is that your nervous system is becoming more reactive—and anxiety is the language it uses.
What Causes Anxiety in Perimenopause?
Perimenopausal anxiety often has a different “signature” than earlier-life anxiety. It can be more body-led, more sudden, and more tied to sleep disruption and stress physiology. This is caused by:
Declining progesterone can reduce the brain’s access to calm. Progesterone supports GABA (the nervous system’s “quieting” neurotransmitter). When it drops, some women notice more tension, a vigilance, or being easily startled.
Fluctuating estrogen can affect serotonin and dopamine—systems involved in mood stability, motivation, and emotional regulation. When estrogen is unpredictable, your emotional baseline can feel less steady.
Cortisol rhythms can shift in midlife, and sleep disruption makes this worse. Many women notice early-morning surges (the “3 a.m. wake-up”) where the body is alert before the mind has a story for it.
Reduced recovery capacity matters. When sleep is lighter, demands are high, and mental load is relentless, your system has fewer resources to return to baseline. Anxiety becomes more likely because your buffer is thinner.
This is why perimenopausal anxiety can feel like: a braced body, a racing mind, a startle response, dread without a clear trigger, or sudden panic that feels “visceral.”
How to Manage Perimenopausal Anxiety
The goal is to help your system become less reactive and more predictable again by:
identifying what kind of anxiety you’re dealing with (hormonal surges vs generalized worry vs panic vs OCD-style loops)
noticing the patterns that amplify anxiety: sleep loss, overstimulation, caffeine/alcohol sensitivity, reassurance seeking, avoidance
building nervous-system supports (grounding, paced exposure, reducing the “all day bracing” state)
strengthening cognitive flexibility—so anxious thoughts are information, not instructions
coordinating with medical care when symptoms suggest sleep interventions or hormonal treatment could be part of the solution
If anxiety is interfering with daily functioning, sleep, relationships, or your sense of safety in your own body, that’s not something you need to power through. It’s a sign you deserve support.
Deeper Dives:
III. Menopause Rage & Irritability

If you’ve found yourself snapping, simmering, or feeling a surge of anger that seems out of character, welcome to perimenopause. This can be one of the most distressing emotional shifts of perimenopause, because it can feel unfamiliar, intense, and hard to control. I hear from clients their thoughts like, “Where on earth is this coming from?” or “I swear, I’m not this kind of person!”
A lot of women feel shame about this. They worry they’re becoming mean, unstable, or “too much.” But irritability and rage in perimenopause are often less about who you are, and more about what your system can no longer tolerate.
Why am I So Angry Now?
Perimenopausal irritability tends to rise when your nervous system has less buffering and your life still demands the same output.
A few overlapping drivers commonly fuel this:
Reduced calming capacity. As progesterone declines, it’s like a loss of the internal “brake” that helps us settle. With less physiological soothing available, irritation can ignite faster and linger longer.
Estrogen volatility. Estrogen fluctuations can affect neurotransmitters that influence mood stability and emotional regulation. That volatility can make your baseline feel less steady, and your reactions more intense.
Sleep disruption and stress physiology. Poor sleep shrinks frustration tolerance. Cortisol changes and chronic stress keep the body in a more reactive state. When you’re already depleted, your bandwidth for “one more thing” becomes very small.
Burnout and emotional labour. By midlife, women have carried years of invisible responsibility: anticipating needs, managing conflict, running the mental load, staying pleasant, staying competent. Perimenopause seems to expose the burden. And when capacity drops, the system stops cooperating with the self-silencing.
Boundary signals. Anger is frequently the emotion that arrives when something has been overridden for too long—needs ignored, limits crossed, or values compromised. In perimenopause, the body is often less willing to keep absorbing what it used to absorb.
This is why perimenopause rage can feel sudden and intense, and also deeply illuminating. It’s physiology interacting with a life that has likely been too heavy for too long.
How Does Therapy Help Perimenopausal Rage?
We don’t need to suppress or judge ourselves. We need to learn what it’s signalling, and to help your nervous system recover enough capacity to respond rather than explode.
To do this, we:
identify your rage pattern (overstimulation, resentment, injustice, depleted caregiving, conflict avoidance, perfectionism)
track what reliably increases reactivity: sleep loss, multitasking, sensory overload, people-pleasing, unspoken needs
build prevention skills (pacing, boundary practice, reducing emotional labour, scheduling recovery)
learn in-the-moment tools (grounding, slowing the escalation curve, repair after rupture)
explore the deeper layer: what your anger has been protecting, and what it needs from you now
If your irritability is impacting relationships, parenting, or your self-respect, or if you’re scared of how intense it feels, support can make a real difference.
Deep Dive:
IV. Depression, Depletion, and Anhedonia
Depression during the menopause transition can feel confusing and frightening. Women who have never struggled with low mood before suddenly find themselves feeling flat, sad, unmotivated, or disconnected from their usual sense of self. Others who have a history of depression may feel old symptoms reappear in ways that feel unfamiliar or harder to manage.
Women often say things like:
“I don’t feel joy the way I used to.”
“Everything feels heavier now.”
“I wake up with a sense of sadness I can’t explain.”
“I feel ungrounded… disconnected from myself.”
“Nothing is wrong, but I’m not okay.”
This can feel alarming, particularly for women who pride themselves on resilience, independence, and emotional strength. But depression in perimenopause is a physiological and psychological response to a system under strain.
Why Do I Feel This Way?
Low mood in perimenopause is often caused by a few factors: biology, sleep, stress physiology, and life context all interact.
Things that contribute include:
Hormonal volatility. Fluctuating estrogen can affect serotonin and dopamine systems involved in mood stability, reward, and motivation. When those systems are less supported, emotional “colour” can fade.
Sleep disruption. Even subtle chronic sleep loss can produce symptoms that mimic depression: reduced pleasure, lower motivation, irritability, slower thinking, and diminished resilience.
Stress load and burnout. When you’ve been carrying too much for too long, the nervous system may shift into a protective state that feels like numbness or shutdown—less emotional range, less spark, less capacity.
Identity and meaning strain. Midlife can surface grief, disillusionment, and role fatigue. When the life you’ve been sustaining no longer fits, the emotional system often signals that misalignment.
Anhedonia. This is the specific experience of reduced ability to feel pleasure or interest. Some women don’t experience menopause-related mood changes as sadness, but as emotional flatness or numbness - it’s often a nervous system and reward system operating with less fuel.
How do I Start to Feel Like Myself Again?
The path forward starts with assessing where you are, as not all low mood needs the same intervention. In therapy, we focus on three questions:
Is this depression, depletion, or both?
What is maintaining it: sleep debt, overfunctioning, isolation, self-criticism, chronic stress?
What restores it: rest, structure, connection, meaning, medical support, or targeted skills?
Supportive therapy work involves rebuilding energy and capacity (pacing, reducing load, restoring sleep), interrupting harsh self-judgment (“why can’t I just snap out of it?”), behavioural activation, and values and meaning work. And importantly, coordinating with medical care when symptoms are persistent, severe, or biologically driven.
If you’ve been feeling low, blank, or unlike yourself for more than a couple of weeks (especially if it’s affecting work, relationships, or your ability to care for yourself) you don’t need to wait until it gets worse to get support.
Deep Dives (read next):
V. Sleep, Exhaustion, and the Emotional & Brain Fog

Hello 3am.
Sleep problems are one of the hallmark symptoms of perimenopause. Even women who have slept well their entire lives suddenly find themselves wide awake at 2:00 a.m., tossing and turning, maybe waking drenched in sweat, or unable to fall back asleep after the slightest disturbance.
Clients describe waking in the night, feeling wired but exhausted, or starting the day already depleted, like their body never truly powered down. And when you’re tired like that, it’s not just your energy that changes. Because sleep is the foundation for emotional regulation, memory, cognitive clarity, and overall resilience, these nighttime disruptions ripple into every corner of a woman’s day.
In particular, brain fog is a common symptom, experienced as forgetfulness, word-finding issues, reduced concentration, and mental fatigue. This is a predictable result of hormonal volatility, stress physiology, and sleep disruption.
Why is it So Hard to Sleep Now?
Sleep is one of the brain’s primary regulators of emotional stability and cognitive functioning. In perimenopause, several biological shifts can make sleep more fragile:
Progesterone decline can reduce the body’s ability to settle into calm, deep rest.
Estrogen fluctuations can affect temperature regulation, mood stability, and the brain systems involved in sleep continuity.
Stress physiology shifts (including cortisol rhythm changes) can increase early-morning alertness—sometimes before you consciously feel anxious.
Vasomotor symptoms (night sweats, temperature swings) can fragment sleep even if you don’t fully wake.
Midlife load matters: when your day is packed with responsibility, the nervous system often stays partially mobilized at night.
Sleep disorders like sleep apnea and restless legs often show up in midlife for women.
Once sleep is disrupted, the downstream effects are predictable:
emotional regulation becomes harder (reactivity rises, recovery slows)
anxiety and irritability increase (the system is more threat-sensitive)
working memory and attention drop (brain fog worsens)
motivation declines (everything requires more effort)
And this is also why perimenopause can feel emotionally overwhelming: when internal resources drop, your capacity to cope shrinks.
Will I Ever Sleep Again?
Hopefully, yes! Therapists trained in Cognitive Behaviour Therapy for Insomnia (the gold standard for treatment of sleep problems), focus on reducing fragmented sleep and protecting nervous-system recovery, because that improves everything else downstream.
Supportive therapy work may include:
identifying what’s disrupting sleep (early waking, rumination, night sweats, anxious body cues, overthinking loops)
strengthening behavioural anchors (consistent wind-down, light exposure timing, caffeine/alcohol sensitivity, pacing)
nervous-system downshifting skills that work in peri (body-first approaches, not just “think calm thoughts”)
CBT-I–informed strategies when insomnia patterns have formed
coordination with medical care when hormonal support or treatment of vasomotor symptoms may improve sleep quality
If you’re exhausted, foggy, and emotionally reactive, it may mean your system is operating without enough repair time. And that is treatable.
A Closer Look:
VI. The Existential Shift: Identity & Grief

One of the hardest parts of perimenopause isn’t a single symptom, but the sense that something is changing inside. You might feel less motivated by what used to drive you. Less willing to perform or over-function. Some women describe it as feeling “unfamiliar” to themselves, or as if the old version of them is harder to access.
This can be disorienting, especially for women who have spent years relying on competence, endurance, and emotional control. If those strategies stop working as well, it’s natural to feel untethered. Am I losing who I was?
My work with perimenopausal women has shown that it’s a shift in identity in midlife, and a grief that comes with it.
What is Happening to Me?
Identity is a story you tell yourself about yourself, and it’s also a lived nervous-system state shaped by hormones, sleep, and stress tolerance. When perimenopause changes your internal baseline, it can change what feels possible, what feels worth it, and what feels aligned.
A few reasons why this may be happening:
Reduced buffering + lower capacity. When you have less internal fuel, you often stop tolerating what you used to tolerate—especially chronic over-responsibility, emotional labour, and misalignment of what matters & your actions.
Motivation systems change. Hormonal shifts can affect dopamine pathways involved in drive and reward. Some women feel less energized by achievement or productivity and more drawn toward meaning, rest, or authenticity.
Emotional sensitivity increases. When your emotional threshold shrinks, certain relationships, roles, or environments may start to feel louder—more obviously draining, unfair, or incompatible.
Midlife reality becomes clearer. Perimenopause often coincides with major life context shifts: aging parents, teenagers, career peak pressure, relationship strain, body changes, accumulated loss. The brain begins integrating these realities differently, which can surface grief.
Grief doesn’t only show up with death. It can be grief for losses and changes like:
a body that feels different than it used to
versions of yourself that were built for survival, performance, or pleasing
years spent carrying too much without support
life paths you didn’t choose (or couldn’t choose)
time—its finiteness, its speed, and what you still want
This is why perimenopause can feel psychologically profound. You’re often more honest with yourself and with reality than you’ve ever been.
How Do I Cope with the Grief and the Changes?
My work with clients has shown me that in midlife, the way forward is to learn what this stage is asking for, and to build a self that fits your current truth and capacity.
Helpful therapeutic approaches:
help you name what has shifted (values, needs, tolerances, identity roles)
identify you grief
work with self-criticism and the fear of disappointing others
strengthen boundaries and reducing emotional labour
rebuild self-trust: “What do I need now?” and “What matters most now?”
support you in making changes gently, without burning your life down
If you’re feeling lost, disconnected, or unusually emotional about aging, identity, or meaning, you don’t need to wait until it becomes a crisis. These are the kinds of concerns therapy is well-suited for—because they deserve language, containment, and support.
A Closer Look:
VII. The Path Forward: Support & Therapy
By the time women reach this point, they’ve been trying to cope for months—or years. They’ve adjusted their expectations, pushed through fatigue, minimized their symptoms, and told themselves they should be able to handle it. And when things still feel hard, the self-blame gets louder: “Why can’t I just get it together?”
If that’s you, hear this: needing support in perimenopause is a normal response to a big transition. Your nervous system is adapting to an internal landscape that has changed, often while your external life continues to demand peak performance. You don’t have to white-knuckle your way through that.
Multi-Layered Support
Perimenopause affects multiple systems at once: hormones, sleep, stress physiology, mood regulation, and cognition. When those systems are shifting together, symptoms often cluster:
disrupted sleep increases anxiety, irritability, and brain fog
chronic stress keeps the body in a vigilant state, reducing recovery capacity
hormonal volatility changes emotional thresholds and motivation
depletion and burnout can mimic depression and blunt pleasure
Because it’s multi-layered, support often needs to be multi-layered too. The most effective approach is usually a coordinated set of stabilizers that reduce reactivity and rebuild capacity. The aim of support is to increase your sense of steadiness during a very nonlinear process.
What Does Support Look Like?
Most women find that they need more than one type of support to get through the transition.
| Support Layer | What It Addresses |
|---|---|
| Physiological (medical) | Hormone therapy, iron, thyroid, and metabolic factors that affect mood, sleep, and energy |
| Sleep restoration | CBT-I strategies, nervous-system downshifting, and medical support for night sweats and temperature disruption |
| Nervous-system support | Reducing overload, building recovery time, improving boundaries, and working with overstimulation |
| Therapy | Anxiety loops, irritability, low mood, identity shifts, grief, and rebuilding self-trust |
The best therapy for perimenopause is done by a clinician who understands the biology, and who can work with the whole picture. That means validating what's changing hormonally while also helping you make real psychological and relational changes. It's rarely one thing that helps; it's the right combination of things, held by someone who knows the difference.
If you want support that’s both validating and practical, and you’re looking for a therapist trained in the perimenopause transition and who can speak to it from experience, you can learn more about working with me here:
Frequently Asked Questions
1) Is this perimenopause — or is something wrong with me?
If you’re noticing new anxiety, irritability, low mood, brain fog, or sleep disruption in your 40s (or earlier/later), perimenopause is a possible contributor, especially if cycles are changing. That said, it’s important to rule out other causes (thyroid issues, iron deficiency, sleep apnea, medication effects, chronic stress/burnout). If symptoms feel sudden, severe, or unlike you, talk with a qualified health-care provider.
2) Can perimenopause cause anxiety or panic even if I’ve never been anxious?
Yes. Many women report body-led anxiety (tight chest, buzzing, dread, sudden panic) emerging during the menopause transition. This can be tied to hormonal fluctuation, sleep disruption, and a more reactive stress system. (Source: BeyondBlue.org)
3) Why does my anxiety feel more physical now?
In perimenopause, anxiety is often driven by nervous-system reactivity: sleep fragmentation, cortisol rhythm shifts, and sensitivity to stimulants (caffeine/alcohol) can make the body feel “on alert” before your mind even catches up. (Source: SOGC Guideline)
4) Does hormone therapy help mood or anxiety?
For some women, particularly those in perimenopause with depressive symptoms, guideline-level evidence suggests hormone therapy may have an antidepressant effect in certain contexts. Decisions about hormone therapy are individual and should be made with a qualified clinician who can assess benefits, risks, and contraindications. (Source: Menopause.org )
5) Should I try antidepressants or therapy, or both?
It depends on the pattern and severity. Psychotherapy is helpful to address anxiety loops, sleep-related spirals, perfectionism/overfunctioning, identity stress, grief, and relationship strain. Medical options can be helpful when symptoms are persistent, severe, or biologically driven. Combined approaches are common and often effective.
6) Is “rage in perimenopause” real, or am I just becoming a difficult person?
It’s real, and it’s common. Irritability often rises when sleep is disrupted, stress load is high, and the nervous system has less buffering. This is frequently a capacity issue (plus, sometimes, long-ignored boundary signals).
7) Is brain fog a sign of dementia?
Brain fog in perimenopause is usually linked to sleep disruption, stress physiology, and hormonal volatility, not dementia. If you’re worried (especially with a strong family history, rapid decline, or significant impairment), speak with your physician for assessment and reassurance.
8) What can I do now while I’m waiting for help?
A useful first step is tracking patterns: sleep quality, cycle changes, stress load, hot flashes/night sweats, caffeine/alcohol effects, and mood shifts. A symptom tracker can help you bring clearer information to medical appointments.
9) When should I seek urgent support?
If you’re having thoughts of self-harm or suicide, or you feel unsafe, seek urgent help immediately (call emergency services, go to your nearest ER, or contact your local crisis line). If you’re in Canada, you can call or text 988 for immediate mental health support.
I'm Kira Hensley, a Registered Psychotherapist in Whitby, Ontario and the founder of Psychotherapy for Her — Durham Region's first psychotherapy practice specializing in perimenopause. I work with women navigating anxiety, self-doubt, and the mental health challenges of midlife, in person and virtually throughout Ontario. Reach out to get started.
Sources & Further Reading
The Menopause Society. Mental Health (patient education).
The Menopause Society. Perimenopause(patient education; includes mood vulnerability discussion).
Society of Obstetricians and Gynaecologists of Canada (SOGC). Guideline No. 422c: Menopause: Mood, Sleep, and Cognition(JOGC).
Beyond Blue. Perimenopause, menopause and mental health (women’s mental health education).
International Menopause Society. Review/summary of NAMS guideline on perimenopausal depression.
The Menopause Society (Menopause journal/clinical guidance PDF). Guideline/position document related to perimenopausal depression.
Menopause Foundation of Canada. Menopause symptom tracker / symptoms resource.
The information on this website is for informational purposes only. It is not intended to be a substitute for professional medical advice, diagnosis, or treatment or to replace your relationship with your health care provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read or seen on this site.